

.png)


What is subtalar fusion (arthrodesis)?
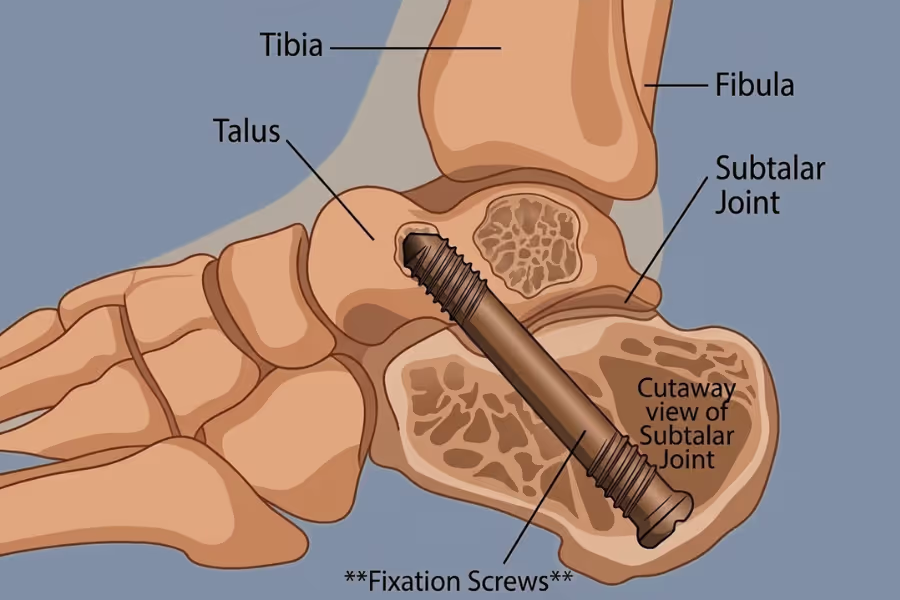
Subtalar fusion (also called a subtalar arthrodesis) is a surgery for the hindfoot that relieves severe pain by permanently joining the heel bone (calcaneus) to the bone right above it (talus).
Think of your foot's joints like a car's suspension system. Your main ankle joint handles the up-and-down motion, but the subtalar joint sits just below it and handles the side-to-side motion. It acts like a shock absorber when you walk on uneven ground. When severe arthritis wears away the cartilage in this joint—often due to wear-and-tear, inflammatory arthritis, or a past heel fracture—the bones grind directly against each other. This causes a deep, constant ache at the back of your foot or below the ankle bone.
What actually happens
- Joint preparation (remove the problem): The surgeon shaves away the remaining damaged cartilage and painful bone spurs to expose healthy, bleeding bone on both sides of the joint.
- Fusion (lock it in place): Instead of trying to preserve the damaged joint, the surgeon tightly locks the two bones together using large titanium screws. Over the next few months, your body heals the two bones together into one solid piece.
Why do it? When clinical exams, X-rays, or an MRI confirm severe subtalar arthritis, a fusion stops the painful grinding. While you will lose some side-to-side tilt in your foot, the up-and-down motion of your main ankle is preserved. For most people, trading a stiff, painful joint for a stiff, pain-free joint is a massive improvement.
Why do Canadians get this surgery done privately?
Shorter wait times
Public waitlists for orthopaedic foot and ankle consults, CT scans, and OR time can be notoriously long—especially because foot arthritis is rarely considered a medical emergency. Private centres can line up assessment and surgery in weeks rather than months, cutting time spent limping, avoiding walks, and dealing with sleep‑killing foot pain.
Choice and control
Going private can let you:
- Pick your surgeon (an orthopaedic foot and ankle specialist) based on hindfoot fusion experience and case volume.
- Schedule around work, exams, caregiving, or travel.
- Get a clear plan regarding the exact hardware to be used and whether bone grafts will be necessary to help the fusion heal.
Peace of mind
You know who’s operating, when it’s happening, and what surgical approach they’ll use. Predictable dates make it easier to arrange time off work and prepare for the strict non-weight-bearing recovery phase.
Preventing further decline
- Function: Ongoing subtalar pain alters the way you walk (causing a severe limp). This puts immense strain on your other joints, leading to secondary pain in your knees, hips, and lower back.
- Joint risk: Severe deformity in the subtalar joint can eventually damage the surrounding healthy joints in the middle of your foot.
- Performance and wellbeing: Faster relief protects your mental health, sleep, and ability to comfortably exercise and work.
Integrated care
Private pathways may offer streamlined imaging, advanced surgical hardware, and coordinated anaesthesia/pain/physio plans—with virtual follow‑ups if you live far away.
Subtalar fusion: what to expect
Typical subtalar fusion often takes about 1.5–2.5 hours of operating time depending on complexity and whether bone grafting is needed. Add time at the centre for check‑in, anaesthesia, and recovery (usually a few extra hours).
Basic steps
1. Check‑in and confirmation
You meet the team, confirm which foot is being operated on, review imaging, and go over the plan. Safety checks are done (including side marking).
2. Anaesthesia
General anaesthesia (you’re fully asleep). Most centres also perform a regional nerve block behind the knee or at the ankle to numb the foot and provide excellent pain control when you wake up.
3. Position and prep
You’re positioned on your side or back. The leg and foot are cleaned and draped sterilely. A tourniquet is usually placed on the calf or thigh to minimize bleeding.
4. Incision and exposure
An incision is made on the outside of the foot, just below the ankle bone. The surgeon gently moves tendons and nerves aside to reach the subtalar joint.
5. Joint preparation
The damaged cartilage is completely scraped out. The surgeon prepares the bone surfaces so they will knit together properly, sometimes packing the area with bone graft (from your own body or a donor) to stimulate healing.
6. Implant placement (Fixation)
The heel is positioned in the perfect alignment for walking. Large titanium screws are then driven through the heel bone and into the ankle bone (talus) to lock the joint tightly together.
7. Rinse and check
The surgeon uses a live X-ray machine (fluoroscopy) to confirm the screws are perfectly placed and the joint is tightly compressed.
8. Close up
Layers are closed with sutures (stitches). The foot is heavily bandaged and placed in a rigid splint or cast to prevent any movement.
9. Wake‑up and instructions
You recover in the post‑anaesthesia care unit, begin gentle movement when safe, and receive strict crutch and weight-bearing instructions. Most patients go home the same day.

What to expect from the recovery process
Every foot is different—follow your surgeon’s plan. A fusion requires the bones to physically heal together, which takes significant time. Steady, smart progress beats pushing too hard.
Week 1
Reality check:
Foot throbbing, heavy swelling, and aching are extremely common. The nerve block will wear off in a day or two, causing a spike in pain.
Goals: Control pain, keep swelling down, and protect the hardware.
Activities: Elevation is critical. Keep the foot elevated above your heart for the vast majority of the day. You will be strictly non-weight-bearing (no weight on the foot at all) using crutches or a knee scooter. Keep the surgical splint completely dry.
Weeks 2–4
Still annoying but improving.
Goals: Wound healing and avoiding flare‑ups.
Activities: You will have a follow-up visit to check the incision and remove stitches. You will likely be placed into a fibreglass cast or a removable walking boot, but you must remain strictly non-weight-bearing. You can move around a bit more, but standing for long periods will cause painful throbbing.
Weeks 5–8
The work phase.
Goals: Confirm bone healing and safely transition to weight-bearing.
Activities: Around the 6-week mark, new X-rays are taken. If the bones are fusing well, your surgeon will gradually allow you to put weight on the foot while wearing the surgical boot. You will start prescribed physio to safely restore strength and mobility to the rest of the foot.
Weeks 9–12
Confidence building.
Goals: Near‑normal daily activity; weaning out of the boot.
Activities: You will transition from the boot to a supportive, stiff-soled running shoe. Walking distances will increase. You may still walk with a slight limp as you regain muscle strength.
Months 3–6+
Back to most normal life.
Goals: Return to usual routines and low-impact sports.
Activities: Add heavier activities only with explicit clearance. Note: Foot swelling after a long day can persist for 6 to 12 months. This is normal.
Helpful tips
- Elevate constantly: If your foot is pointing down in the first two weeks, it will throb intensely.
- Knee scooter: A knee scooter is much safer and less exhausting than crutches for the long non-weight-bearing phase.
- Bowel plan: Pain meds can constipate—hydrate and use fibre/stool softeners if needed.
- Respect the timeline: Walking on the foot too early can snap the screws or cause a "non-union" (the fusion fails to heal).
Red flags—call your care team
- Fever, spreading redness, or foul drainage from the incision.
- Calf pain, swelling, or tenderness behind the knee (signs of a potential blood clot).
- Severe, worsening pain that medication cannot touch.
- Toes that become completely numb, freezing cold, or turn blue.
How much does subtalar fusion surgery cost in Canada?
Exact prices depend on whether bone grafts are needed, the specific titanium hardware used, and the surgical facility. Always ask for a written, itemized quote.
Cost in Canada (private)
Typical range: $10,000 - $18,000+
Cost in the United States
Typical range: CA$15,000 - CA$35,000+
What’s usually included
- Surgeon fee and anaesthesia services.
- The surgical hardware/implants (large titanium screws) and basic bone graft materials.
- Accredited facility/OR time, nursing, and standard disposables.
- Basic intra‑op imaging (fluoroscopy) and routine supplies.
- Immediate recovery care (PACU) and early follow‑up visit(s).
What’s often not included
- Initial consults and pre‑op imaging (CT scans, X‑rays) done outside the clinic.
- Specialized mobility aids (knee scooters, crutches) or custom surgical boots.
- Complex bone grafts (if you need a large piece of bone taken from your hip to fill a defect).
- Prescriptions after discharge (pain, nausea, blood thinners).
- Post‑op physiotherapy.
- Travel and accommodation if you’re out‑of‑province/state.
Tips to compare quotes
Ask if it’s a global bundle and request line items for: surgeon, facility, anaesthesia, implants (hardware cost), imaging, follow‑ups, and what triggers extra charges (e.g., if they need to harvest bone from your pelvis during the surgery).
How to choose a surgeon and clinic
Choosing your surgeon is a major benefit of pursuing private surgery. Here’s how to choose wisely for a subtalar fusion.
What to look for
Experience and volume (foot and ankle specific)
Ask how many hindfoot or subtalar fusions they do each year.
Fusing the subtalar joint is highly "precision-dependent" because:
- the heel must be locked into the exact right alignment (fusing it tilted too far inward or outward will ruin how you walk).
- the bone ends must be prepared perfectly to ensure they heal together (fuse) completely.
- they must distinguish between subtalar arthritis and arthritis in the surrounding joints.
Also ask about their case mix:
- Isolated subtalar fusion vs. triple arthrodesis (fusing three joints in the back of the foot at once).
- Arthroscopic vs. open surgery (some surgeons can do this through tiny camera holes; others need a larger incision depending on the joint damage).
Credentials and training
- Verify licensure with your provincial college (CPSO Ontario, CPSBC BC, CPSA Alberta, CMQ Québec, etc.).
- Look for FRCSC-certified orthopaedic surgeons with fellowship training in foot and ankle surgery.
- Bonus: Surgeons who regularly treat complex foot deformities or participate in foot and ankle societies.
For a more in-depth guide read, How to Understand Surgeon Credentials in Canada
Outcomes and safety (ask for real numbers)
Request recent data, ideally for foot fusions specifically:
- Non-union rate: (How often do the bones fail to heal together, requiring a second surgery?)
- Infection rate: (Foot wounds are further from the heart and can be slower to heal).
- Nerve injury: (Temporary or permanent numbness on the side of the foot).
- Hardware removal rate: (How often do the large heel screws irritate the tissue so much they need to be taken out later?)
Clear indications and alternatives
Make sure they confirm you’re a good candidate for a fusion.
A careful surgeon should explicitly assess:
- whether your pain is truly coming from the subtalar joint (side-to-side motion) rather than the main ankle joint (up-and-down motion).
- whether you have severe deformity (like a flat foot that has completely collapsed) that requires fixing other bones at the same time.
- whether your bone quality is healthy enough to hold the metal screws.
They should also compare a fusion to:
- custom orthotics, rigid ankle braces, and cortisone injections.
Surgical plan and implant strategy
Ask:
- Will this be done open or arthroscopically (with a camera)?
- Will you need to use a bone graft (taking bone from my hip, shin, or a donor) to help the joint fuse?
- What hardware do you use (e.g., one or two large screws through the heel)?
Imaging and planning (must be thorough)
Good programs use imaging to confirm candidacy:
- Weight-bearing X-rays to see how your foot aligns when you stand on it.
- CT scan (highly recommended) to look at the exact 3D shape of the joint and measure bone health.
- MRI or diagnostic injections (numbing the joint) to absolutely confirm the subtalar joint is the true source of your pain.
Facility accreditation and safety systems
Choose accredited centres (e.g., Accreditation Canada / CAAASF) with:
- modern fluoroscopy (live X-ray) to ensure perfect screw placement during surgery.
- experienced anaesthesia teams skilled in regional foot/leg nerve blocks (crucial for pain control).
- a clear transfer pathway to a hospital if needed.
Rehab integration (bone healing requires strict protocols)
You want a written plan for:
- weight-bearing status (you will likely be strictly off the foot for 6 weeks).
- cast and walking boot timeline.
- physiotherapy timeline (safe transition to walking).
Transparent pricing (hardware and biologics matter)
Request an itemized quote including:
- surgeon fee
- facility/OR fees
- anaesthesia
- implant/hardware cost (titanium screws).
- bone graft materials (if synthetic or donor bone is needed, this can be expensive).
- imaging/fluoroscopy
- follow-ups (and whether virtual follow-ups are included)
Questions to ask at your subtalar fusion consultation
Surgeon and plan
- How many subtalar fusions do you perform yearly?
- Do I need a bone graft, and if so, where will you take the bone from?
- Are my other foot joints healthy, or will they need to be fused in the future too?
Technique and safety
- What is your non-union (failed fusion) rate?
- Will you do this through a large incision or tiny camera holes?
Recovery and after-care
- How long must I be strictly non-weight-bearing (on a scooter/crutches)?
- When can I drive (if it’s your right foot) and return to my specific job?
- What symptoms should prompt an urgent call (calf pain, tight cast, freezing toes)?
Costs and logistics
- What exactly is included in my quote (especially the screws and bone graft)?
- How are follow-ups and X-rays handled if I live out of province?
Signals of a high-quality foot fusion program
- Performs hindfoot fusions regularly and thoroughly explains the difference between the subtalar and ankle joints.
- Shares complication rates (like non-union) openly and sets extremely realistic expectations about the long, strict recovery.
- Operates in an accredited facility with experienced anaesthesia and emergency pathways.
- Provides a written, phased recovery plan focused on safe bone healing.
- Offers transparent, itemized pricing—including the hardware and bone graft costs.
If you're currently interested in private surgical pathways within Canada, you can click here for a list of providers.

Subtalar fusion - frequently asked questions
How do I know this surgery is right for me?
Subtalar fusion is a specific solution for end-stage arthritis or severe deformity in the hindfoot. It is right for patients who suffer from deep, daily heel/ankle pain and are willing to permanently trade the side-to-side tilting motion of their foot for a stable, pain-free joint.
Signs a subtalar fusion might be right for you
- Walking on uneven ground is agony: Walking on grass, gravel, or slanted sidewalks causes sharp, deep pain below your ankle.
- Severe stiffness: Your foot already refuses to tilt side-to-side due to arthritis or a past injury (like a broken heel bone).
- Failed conservative care: Custom orthotics, stiff-soled shoes, bracing, and cortisone injections no longer provide relief.
- Diagnostic clarity: A CT scan or X-ray confirms "bone-on-bone" grinding in the subtalar joint.
When it might not be the right option (or other treatments are better)
- The pain is in the ankle joint: If your pain comes from the main up-and-down hinge of the ankle, you need an ankle fusion or replacement, not a subtalar fusion.
- Mild arthritis: If you still have good cartilage and conservative treatments work, it is usually best to wait.
- You are a heavy smoker: Nicotine destroys the bone's ability to fuse. Many surgeons will refuse to operate until you quit, as the failure rate is too high.
When to get assessed sooner
- Rapid foot collapse: If your foot is quickly changing shape (becoming severely flat or tilted), delaying can damage the surrounding joints, requiring a much larger surgery later.
- Severe altered gait: If you are limping so badly that your knee, hip, or lower back is now in constant pain.
Do I need a referral?
Yes and no—you can reach out to any of the private surgeons listed on Surgency without a referral. Their intake teams are happy to answer questions, explain what they treat, share pricing ranges, and walk you through next steps.
However, to book a formal consultation with the surgeon, you'll typically need a referral from your family doctor or nurse practitioner. Don't have one? Many of the clinics can help coordinate a virtual GP appointment to get the referral paperwork sorted. All surgeons listed on Surgency offer virtual initial consultations, so you don't need to travel until you and the surgeon have agreed on a plan.
Before your consultation, expect the clinic to request relevant medical records and recent diagnostic imaging (X-ray, MRI, CT, ultrasound, lab work, etc.). Having these ready speeds up the process and lets the surgeon give you specific guidance on your very first call.
How do I prepare for surgery?
Your surgeon’s instructions come first—follow their plan if it differs.
Prehab and health optimization
Prepare your upper body and "good" leg
- You will be completely off your surgical foot for 6 to 8 weeks. Work on your upper body, core, and good leg strength now to handle crutches or a knee scooter.
Quit nicotine
- Crucial for bone fusion: The two bones must grow into each other to be successful. Nicotine severely chokes off the blood supply needed for bones to heal. Smoking dramatically increases the risk of a "non-union" (the fusion failing) and wound infections. Stop 4 to 6 weeks before surgery.
Medication review
- Share all prescriptions, OTC meds, and supplements.
- Pause blood thinners and anti‑inflammatories as directed (NSAIDs can sometimes interfere with bone healing).
Home prep
Safe layout
- Clear clutter and remove loose rugs to prevent tripping while on crutches/scooter.
- Set up a “recovery zone” on the main floor with essentials (water, meds, phone charger) easily reachable without standing up.
Mobility aids and elevation
- Rent or buy a knee scooter. It is a lifesaver for getting around the house while remaining non-weight-bearing.
- Gather firm pillows. You must keep your foot elevated above your heart constantly for the first 1–2 weeks to control the intense throbbing.
Bath setup
- Non‑slip mat and a shower chair (balancing on one foot in a wet shower is dangerous).
- Get a waterproof cast cover or large garbage bags/tape to keep your splint/cast completely dry.
Clothing
- Baggy pants or shorts: Your leg will be wrapped in a bulky cast or splint up to your knee. Normal pants will not fit over it.
Food, meds, and surgery‑day prep
Meal prep
- Pre-cook and freeze meals. Standing at the stove on one leg is exhausting and painful early on.
Constipation plan
- Pain meds slow the gut; have stool softeners and hydration ready.
Skin prep
- Use the antiseptic wash as directed.
- Do not shave your foot or leg yourself to avoid micro-cuts, which carry an infection risk.
What to bring
- Health card/ID, medication list, and imaging.
- Loose clothing for the ride home.
- Your knee scooter or crutches.
Red flags to know
- Calf pain: Severe pain, swelling, or heat in the calf behind your knee (potential blood clot).
- Cast issues: If your toes become freezing cold, numb, or blue, the cast/splint is too tight.
- Wound issues: Spreading redness, foul drainage, or a sudden spike in pain under the cast.
- Chest pain or shortness of breath: Requires immediate emergency care.
How much does Surgency cost?
Surgency is free for patients, funded for by surgeons.
Surgeons—who meet our listing criteria—pay a flat fee to list on the Surgency platform. To maintain objectivity, there are no commissions, referral fees, nor any ranking or recommending one surgeon over another.
Surgency is patient-first. Our goal is to make the process of finding a private surgeon as simple as possible. You choose who to contact. Learn more in our Advertising Policy.
What are the risks involved with surgery?
Your personal risk depends on your bone quality, whether you smoke, and your general health. Discuss your specific risks with your surgeon.
Common and usually temporary
- Foot swelling: Swelling is entirely normal and can persist for 6 to 12 months after major foot surgery.
- Throbbing pain when standing: In the early weeks, every time you lower your foot to the ground, blood rushes in and causes intense throbbing. Elevation is mandatory.
- Transfer pain: As you adjust to walking without side-to-side foot motion, you may temporarily feel new aches in your knee or midfoot.
Less common
- Non-union (bones fail to fuse): The most specific risk for this surgery. If the bones do not knit together into one solid piece, you will continue to have pain and the screws may break. This requires a second surgery and bone grafting. (Risk is much higher in smokers and diabetics).
- Hardware irritation: The large screws inserted through the heel can sometimes irritate the fat pad on the bottom of your foot. They can be removed in a minor surgery after the bone has fully fused (usually after a year).
- Infection: Risk is low but serious. It can occur at the incision site or, rarely, deep in the bone.
Procedure-specific considerations (Subtalar Fusion)
- Malunion (fused at the wrong angle): If the heel is fused tilted too far inward or outward, it alters your foot mechanics and can cause chronic pain.
- Adjacent joint arthritis: Because the subtalar joint no longer absorbs side-to-side shock, the joints in the middle of your foot have to work harder. Over many years, this can lead to new arthritis in those neighboring joints.
Uncommon but important
- Nerve damage: The sural nerve runs near the outside of the foot. It can be stretched or injured, leading to permanent numbness on the outside edge of the foot or chronic nerve pain.
- Blood clots (DVT): Reduced mobility and casting increase clot risk. You may be prescribed blood thinners after surgery.
- Complex Regional Pain Syndrome (CRPS): A rare nervous system overreaction causing severe, ongoing foot pain, swelling, and skin color changes.
How you can lower risk
- Stop nicotine completely: This is the single best way to prevent a non-union and wound infection.
- Obey the weight-bearing rules: Do not put any weight on the foot until your surgeon explicitly says the X-rays show it is safe.
- Elevate constantly: Keeping the foot above the heart drastically reduces swelling, throbbing, and cast tightness.
What are the risks of delaying or not pursuing surgery?
Your situation depends on how bad your daily pain is, whether your foot is changing shape, and how fast the arthritis is progressing.
Main risks of delaying (when symptoms are significant)
Severe joint destruction and deformity
- As the cartilage disappears, the bones grind and collapse. Your foot may start to severely flatten out or tilt permanently. If the deformity becomes too severe, a simple subtalar fusion is no longer enough; you may need a massive surgery (triple arthrodesis) to rebuild the entire back of the foot.
Compensatory pain (Kinetic chain issues)
- A painful, stiff hindfoot forces you to walk with a severe limp. Over months and years, this abnormal walking causes painful wear-and-tear in your knees, hips, and lower back.
Damage to surrounding joints
- If the subtalar joint collapses, it puts unnatural stress on the healthy joints in the middle of your foot and your main ankle, accelerating arthritis in those areas.
Loss of mobility and fitness
- Avoiding walking or exercising due to deep foot pain leads to cardiovascular decline, weight gain (which puts more stress on the foot), and muscle atrophy.
When watchful waiting can be reasonable
- Your pain is mild and only happens after walking on very uneven ground (like hiking).
- Custom orthotics and stiff-soled shoes successfully manage your daily symptoms.
- You are willing to modify your lifestyle to avoid activities that stress the joint.
When not to delay (seek prompt assessment)
- Rapid foot collapse: You notice your arch has suddenly fallen, or your heel is aggressively tilting outward.
- Severe altered gait: You are limping so badly that your knees and hips are failing.
- Inability to walk: The pain prevents you from completing basic, necessary daily tasks.
I still have questions
If you still have questions, please feel free to contact us directly.
Please note: Surgency is not a clinic itself. Nor can we help with emergency situations, or provide personalized medical advice—that is between you and your surgeon. If you are experiencing acute or severe symptoms, please present to your local emergency department or urgent care centre.
.avif)


