

.png)



What is biceps tenodesis?
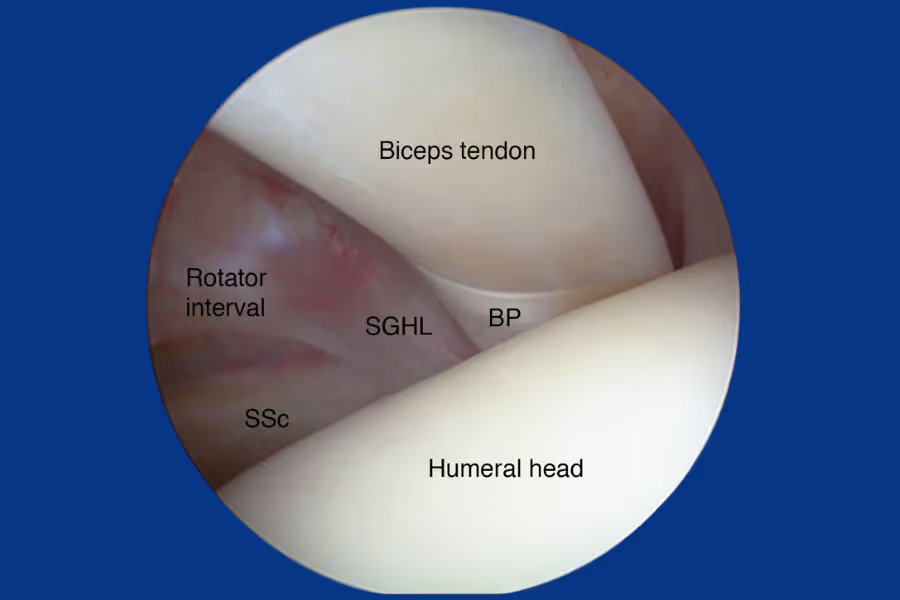
Biceps tenodesis is a surgery for the shoulder that treats pain and dysfunction caused by damage to the long head of the biceps tendon (LHBT)—the tendon that connects the top of your biceps muscle to the shoulder socket (specifically, the labrum and the top of the glenoid).
Think of the long head biceps tendon like a rope anchored to the top of your shoulder socket. Over time—or after an injury—that rope can fray, partially tear, become inflamed (tendonitis), or slip out of its groove (subluxation). When this happens, you get pain in the front of the shoulder, aching down the upper arm, and weakness with lifting or overhead movements. The biceps tendon is also commonly involved when the labrum tears at the top of the socket (a SLAP tear).
What actually happens
- Detach: The surgeon cuts the damaged biceps tendon from its attachment at the top of the shoulder socket (labrum).
- Reattach (tenodesis): The tendon is moved to a new anchor point on the humerus (upper arm bone), either in the bicipital groove or just below the shoulder joint. It's secured using a small screw, button, or suture anchor drilled into the bone.
- Result: The biceps muscle keeps working normally—you maintain arm contour, strength, and function—but the damaged, pain-generating attachment in the shoulder is eliminated.
Open vs. arthroscopic
Biceps tenodesis can be performed arthroscopically (through small keyhole incisions with a camera), as a mini-open procedure (small incision near the front of the shoulder or upper arm), or as a subpectoral open procedure (incision in the armpit crease). Your surgeon will choose the technique based on where the tendon damage is and what other shoulder work is needed.
Why do it? When shoulder pain from biceps tendon damage persists despite rest, physio, and injections—especially if it's affecting sleep, work, sport, or daily activities—biceps tenodesis offers a reliable way to eliminate the pain source while preserving the muscle's strength and appearance.
Why do Canadians get this surgery done privately?
Shorter wait times
Shoulder surgery often faces lengthy queues for consultation, imaging (MRI), and OR time. Instead of waiting months, private centres can schedule surgery within weeks—reducing time spent with front-of-shoulder pain, night pain, and activity restrictions, and helping you return to work, sport, or daily life sooner.
Choice and control
Going private can let you:
- Pick your surgeon based on shoulder arthroscopy and biceps tenodesis experience and credentials
- Select the clinic location (often out-of-province)
- Plan surgery around work, competitive seasons, or family schedules
Peace of mind
You know who's operating, when it's happening, and the detailed plan (fixation technique, concomitant procedures, rehab milestones). Clear timelines reduce anxiety and help families and employers coordinate support.
Preventing further decline
- Function and performance: Limits months of pain, weakness, and restricted overhead use that derail work, sport, and sleep
- Joint health: Ongoing biceps instability or SLAP pathology can worsen rotator cuff wear and shoulder mechanics; earlier intervention can protect the joint
- Surgical complexity: Chronic tendon damage and retraction can make later surgery more difficult
- Mental load: Shortens time living with uncertainty, restricted activities, and poor sleep from night symptoms
Integrated care
Private pathways may offer streamlined imaging, coordinated surgical and rehab plans, and virtual follow-ups if you live far away.
Biceps tenodesis: what to expect from the surgery process
Biceps tenodesis typically takes about 45–90 minutes of operating time when performed as an isolated procedure. When combined with other shoulder work (rotator cuff repair, labral debridement, subacromial decompression), total time may be 1.5–2.5 hours. Expect a few extra hours at the centre for check-in, anaesthesia, and recovery before heading home. This is almost always a same-day (outpatient) procedure.
Basic steps
1. Check-in and marking
You meet the team, the surgeon marks the shoulder, and you review the plan.
2. Anaesthesia
You'll get general anaesthesia (asleep) and often a nerve block (interscalene block) to numb the shoulder and arm for pain control after surgery.
3. Position and prep
You're positioned safely (beach-chair or lateral). The skin is cleaned and covered with sterile drapes.
4. Diagnostic look (arthroscopy)
The surgeon inserts a small camera through keyhole incisions to inspect the shoulder joint—confirming the biceps tendon damage and checking the rotator cuff, labrum, and cartilage.
5. Biceps tendon release
The damaged tendon is cut from its attachment at the top of the shoulder socket (labrum).
6. Tenodesis (reattachment)
The tendon is pulled to its new position on the humerus. A small hole or socket is prepared in the bone, and the tendon is secured with an interference screw, suture anchor, or button fixation device. The surgeon sets the correct tension so the biceps muscle functions normally.
7. Additional work (if needed)
If there's a rotator cuff tear, labral damage, bone spurs, or impingement, these are addressed in the same session.
8. Close up
Small incisions are closed with stitches or strips, covered with a dressing, and a sling is fitted.
9. Wake-up and instructions
You recover in the post-anaesthesia care unit, get discharge instructions for the sling and early movement, and head home the same day.
What to expect from the recovery process
Every shoulder is different—follow your surgeon's plan. Taking rehab seriously usually means better results. Some private clinics offer virtual follow-ups or coordinate physio near home.
Week 1
Reality check: Soreness, swelling, stiffness, and tough sleep. Not fun. The nerve block may keep the arm numb for a day.
Goals: Control pain and swelling, protect the repair, start safe motion.
Activities: Wear the sling as directed (typically 3–4 weeks). Ice and elevate. Keep the incision clean and dry. Move fingers, wrist, and elbow. Gentle pendulum exercises if cleared by your surgeon. A helper is useful for dressing, meals, and medication.
Weeks 2–4
Still annoying but improving.
Goals: Gradually restore pain-free range of motion (ROM) within limits; stay safe in the sling.
Activities: Regular physio begins. Passive to assisted ROM (forward elevation and external rotation to set limits). Scapular setting exercises. Light daily tasks at waist level. No active biceps curling, no resisted elbow flexion, and no forearm supination against resistance for at least 6 weeks—this protects the healing tenodesis.
Weeks 5–8
The work phase.
Goals: Wean from sling (as cleared). Near-full ROM by ~8 weeks. Begin gentle strengthening.
Activities: Start gentle active ROM. Initiate resisted biceps curls and supination only when cleared (usually around 6 weeks). Rotator cuff and scapular strengthening with light resistance bands. Posture work. Controlled functional use below shoulder height.
Weeks 9–16
Building strength and confidence.
Goals: Full ROM, better strength and endurance, stable shoulder with everyday use.
Activities: Progress resistance exercises (biceps, rotator cuff, deltoid, scapula). Closed-chain work (wall/plank variations). Coordination and sport-prep drills (no contact or heavy overhead yet). Low-impact cardio as cleared.
Months 4–6
Return to full activity.
Goals: Power, endurance, and trust in the shoulder.
Activities: Sport-specific and work-specific drills. Gradual return to overhead work, heavy lifting, and contact sports only when cleared by your surgeon and physio. Full recovery typically takes 4–6 months.
Helpful tips
- Protect the tenodesis: The biggest early risk is stressing the repair with biceps curling or heavy gripping. Be patient.
- Sleep: A recliner or propped-up position is often more comfortable than lying flat for the first few weeks.
- Ice often: Helps with pain and swelling, especially in the first week.
- Physio matters: Consistent rehab is the biggest factor in getting your strength and motion back.
Red flags—call your care team
- Fever, increasing redness/drainage from the incision.
- Severe calf pain/swelling, chest pain, or shortness of breath.
- New numbness or weakness in the hand or fingers.
- A sudden "pop" or visible change in biceps muscle shape (possible tenodesis failure).
How much does biceps tenodesis surgery cost in Canada?
Exact prices depend on whether biceps tenodesis is performed as an isolated procedure or combined with rotator cuff repair, labral work, or subacromial decompression, and where you have it done. Combined procedures cost more. Always ask for a written, itemized quote.
Cost in Canada (private)
Typical range: $8,000 - $20,000+
Note: Costs increase when tenodesis is combined with rotator cuff repair or other shoulder procedures. Some centres offer bundled pricing.
Cost in the United States
Typical range: CA$12,000 - $35,000+
Varies widely by setting (ambulatory surgery centre vs. hospital), state, and whether additional procedures are performed.
What's usually included
- Surgeon and anaesthesiologist fees.
- Facility/OR time, nursing, and standard disposables.
- Fixation hardware (interference screw, suture anchor, or button).
- Nerve block and immediate post-op care.
- Sling and standard dressings.
- Basic follow-up visit(s) right after surgery.
What's often not included
- Pre-op imaging (X-rays, MRI) and specialist consults done externally.
- Additional or premium implants/anchors beyond a standard bundle.
- Long-term physiotherapy after the first visit(s).
- Prescription medications after discharge.
- Travel and accommodation if surgery is out-of-province/state.
- Treatment of complications outside the normal "global" period.
Tips to compare quotes
Ask if it's a global bundle and request line items for: surgeon, facility, anaesthesia, implants/hardware, nerve block, imaging review, sling, and follow-ups, and what triggers extra charges (e.g. if rotator cuff repair or labral work is added once the surgeon is in the joint).
Insurance and financing options
- Private health insurance: Some plans may cover part of the costs. Check your policy directly.
- Financing plans: Many clinics offer monthly payment options to help spread out the cost. Learn more about your financing options here.
- Medical Expense Tax Credit (METC): This is a non-refundable credit that reduces your taxes when you pay out-of-pocket for eligible medical expenses. Learn more about how to claim METC for private surgeries.
How to choose a surgeon and clinic
Choosing your surgeon is one of the biggest benefits of going private—use it to your advantage.
What to look for
Experience and volume (biceps tenodesis-specific)
Ask how many biceps tenodesis procedures they perform per year, and their case mix:
- Isolated tenodesis vs. combined with rotator cuff repair or SLAP debridement
- Arthroscopic vs. mini-open vs. subpectoral technique—and why they prefer their approach
- Experience with younger/athletic patients vs. older/degenerative cases
Higher volume and routine outpatient pathways usually correlate with smoother care and fewer complications.
Credentials and training
- Verify licensure with your provincial college (CPSO Ontario, CPSBC BC, CPSA Alberta, CMQ Québec, etc.)
- Look for FRCSC-certified orthopaedic surgeons** with fellowship training in shoulder & elbow or sports medicine/upper-extremity surgery
- Bonus: surgeons who regularly teach, publish outcomes, or participate in shoulder surgery societies
For a more in-depth guide read, How to Understand Surgeon Credentials in Canada
Outcomes and safety (ask for real numbers)
Request recent data:
- Tenodesis failure/re-tear rate
- Infection rate
- Nerve irritation or injury rate
- Persistent pain or stiffness rate
- Unplanned return to OR within 30–90 days
- Patient-reported outcomes: pain relief, function scores (ASES, Constant), return-to-work/sport timelines, and satisfaction
Clear indications and alternatives
A careful surgeon should:
- Confirm the biceps tendon is the primary pain generator (not just an incidental finding on MRI)
- Explain tenodesis vs. tenotomy and why one is better for you
- Discuss whether concomitant procedures are needed (rotator cuff repair, subacromial decompression, labral work)
- Compare surgery to continued non-operative management if you're still improving
Surgical plan and fixation
Ask:
- Technique: Arthroscopic, mini-open, or subpectoral? Why for you?
- Fixation: Interference screw, suture anchor, or button? What evidence supports their choice?
- Tendon tension: How do they set correct biceps tension to avoid cramping or cosmetic changes?
- Concomitant procedures: What else might they address if they find additional pathology during arthroscopy?
Imaging and planning
- Pre-op MRI to evaluate the biceps tendon, labrum, rotator cuff, and cartilage
- X-rays to rule out bony issues
- Correlation of imaging with your symptoms and physical exam findings
Facility accreditation and safety systems
Confirm the clinic is accredited (e.g. Accreditation Canada / CAAASF) with shoulder-appropriate equipment, experienced anaesthesia, and trained staff.
Rehab integration
A written, phased rehab protocol with clear timelines for:
- Sling use and early motion
- When to begin resisted biceps work (critical—too early can fail the repair)
- Return to desk work, manual work, sport
- Coordination with a local physiotherapist if you're travelling
Transparent pricing
Request an itemized quote including:
- Surgeon fee
- Facility/OR fees
- Anaesthesia and nerve block
- Implants/hardware
- Sling
- Follow-up visits
Clarify what triggers additional charges (e.g. adding rotator cuff repair, extra anchors, longer OR time).
Questions to ask at your biceps tenodesis consultation
Surgeon and plan
- How many biceps tenodesis procedures do you perform yearly?
- Do you recommend tenodesis or tenotomy for me—and why?
- Will you address any other shoulder pathology at the same time?
Technique and safety
- Which technique and fixation do you prefer and why?
- What are your rates of tenodesis failure, infection, and nerve complications?
- How do you set the correct biceps tension?
Recovery and aftercare
- How long will I wear a sling?
- When can I start biceps strengthening?
- What's my expected timeline to return to desk work, manual work, and sport?
- Do you provide a written rehab protocol for my physio?
Costs and logistics
- What exactly is included in my quote?
- What could add cost (additional procedures, extra implants, complications)?
- How are follow-ups handled if I live out of province?
Signals of a high-quality private program
- Performs biceps tenodesis regularly and explains tenodesis vs. tenotomy clearly
- Shares outcomes data and complication rates openly
- Provides a written, phased rehab protocol with clear return-to-activity timelines
- Offers itemized, transparent pricing with what's included and excluded
- Coordinates with your local physiotherapist and provides direct post-op contact details
- Operates in an accredited facility with shoulder-appropriate equipment
If you're currently interested in private surgical pathways within Canada, you can click here for a list of providers.

Biceps tenodesis - frequently asked questions
How do I know this surgery is right for me?
Biceps tenodesis is specifically designed to eliminate pain from the long head biceps tendon while preserving the muscle's strength and appearance.
Signs biceps tenodesis might be right for you
- Front-of-shoulder pain that won't quit: Aching or sharp pain at the front of the shoulder or down the upper arm, especially with overhead reaching, lifting, or pulling.
- Failed conservative treatment: You've tried physio, rest, anti-inflammatories, and possibly injections without lasting relief.
- Biceps tendon damage on MRI: Partial tear, fraying, subluxation (tendon slipping out of its groove), or tendonitis confirmed on imaging and matching your symptoms.
- SLAP tear with biceps involvement: Your labrum is torn at the top of the socket and the biceps anchor is compromised.
- You're active or care about arm appearance: Tenodesis preserves biceps contour and strength better than tenotomy—preferred for younger patients, athletes, labourers, and anyone who wants to avoid the "Popeye" deformity.
- Combined with rotator cuff repair: Biceps tenodesis is frequently performed alongside rotator cuff surgery when the tendon is damaged.
When tenotomy might be better
- Older, less active patients: Tenotomy (simply cutting the tendon and letting it retract) is a simpler procedure with faster initial recovery. It may be appropriate if arm contour and maximum strength preservation are less important to you.
- Lower physical demands: If you don't do heavy overhead work or sport, tenotomy may provide equivalent pain relief with a quicker recovery.
When to get assessed sooner
- Shoulder pain is affecting your sleep, work, or ability to exercise.
- You notice weakness with lifting or overhead movements.
- You feel or hear a "popping" or "clicking" in the front of the shoulder.
- You've had a sudden injury and notice a visible change in your biceps muscle contour.
Do I need a referral?
Yes and no—you can reach out to any of the private surgeons listed on Surgency without a referral. Their intake teams are happy to answer questions, explain what they treat, share pricing ranges, and walk you through next steps.
However, to book a formal consultation with the surgeon, you'll typically need a referral from your family doctor or nurse practitioner. Don't have one? Many of the clinics can help coordinate a virtual GP appointment to get the referral paperwork sorted. All surgeons listed on Surgency offer virtual initial consultations, so you don't need to travel until you and the surgeon have agreed on a plan.
Before your consultation, expect the clinic to request relevant medical records and recent diagnostic imaging (X-ray, MRI, CT, ultrasound, lab work, etc.). Having these ready speeds up the process and lets the surgeon give you specific guidance on your very first call.
How do I prepare for surgery?
Your surgeon's instructions come first—follow their plan if it differs.
Prehab and health optimization
Shoulder "prehab"
- If cleared, work with your physio on scapular strengthening and rotator cuff activation before surgery. A stronger shoulder going in often means a smoother recovery.
- Maintain a daily walking habit—better cardiovascular health improves healing.
Quit nicotine
- Smoking and nicotine impair tendon healing and increase infection risk. Stop 4+ weeks before surgery.
Medication review
- Share all prescriptions, OTC meds, and supplements with your surgeon.
- Pause blood thinners and anti-inflammatories as directed.
Home prep
Safe layout
- Set up a recovery zone with essentials at waist height so you can reach things one-handed.
- Move frequently used items to counter level.
Clothing
- Button-up or zippered tops are much easier than pulling shirts over your head while in a sling. Practise dressing one-handed before surgery.
Sleep setup
- Many people find sleeping in a recliner or propped up with pillows more comfortable than lying flat for the first 2–3 weeks.
Food and supplies
- Pre-make or stock easy meals (microwavable, one-handed options).
- Have ice packs ready (frozen peas work well).
- Fill prescriptions in advance if possible.
Day-of prep
- Follow fasting instructions exactly (no food or drink after midnight or as directed).
- Use antiseptic wash as instructed.
- Wear loose, comfortable, front-opening clothing.
- Remove jewellery, piercings, and contact lenses.
- Bring health card/ID, medication list, and imaging.
- Arrange a ride home and a helper for the first 1–2 days.
Practice ahead
- Practice getting dressed, opening containers, and basic tasks one-handed.
- Set up short walking routes for post-op mobility.
How much does Surgency cost?
Surgency is free for patients, funded for by surgeons.
Surgeons—who meet our listing criteria—pay a flat fee to list on the Surgency platform. To maintain objectivity, there are no commissions, referral fees, nor any ranking or recommending one surgeon over another.
Surgency is patient-first. Our goal is to make the process of finding a private surgeon as simple as possible. You choose who to contact. Learn more in our Advertising Policy.
What are the risks involved with surgery?
Your personal risk depends on the extent of surgery (isolated tenodesis vs. combined with rotator cuff repair), fixation technique, and your general health. Discuss your specific risks with your surgeon.
Common and usually temporary
- Soreness and stiffness: Expected for the first several weeks. The nerve block wears off in 12–24 hours, and pain is managed with medication.
- Swelling and bruising: Normal around the shoulder and upper arm. Gravity may cause bruising to track down toward the elbow.
- Stiffness: Some degree of shoulder stiffness is common early on and improves with physio.
Less common
- Tenodesis failure (loss of fixation): The tendon can pull out of the bone before it fully heals, especially if resisted biceps work starts too early. Risk is generally low (under 5%) but varies with technique and compliance.
- Persistent bicipital groove pain: Ongoing discomfort at the fixation site. Usually settles over time.
- Infection: Risk is generally low with arthroscopic/mini-open approaches.
- Nerve irritation: Temporary numbness or tingling around the incision or in the arm. Rarely permanent.
- Stiffness/frozen shoulder: Uncommon but possible if motion is not restored progressively.
Uncommon but important
- Proximal humerus fracture: Very rare, but reported with certain fixation techniques (especially interference screws). Risk is higher in patients with weaker bone.
- Popeye deformity: If the tenodesis fails, the biceps muscle can bunch up, creating a visible bulge (similar to what happens with tenotomy). May require revision.
- Biceps cramping: Occasional cramping in the biceps muscle, especially with heavy use. Usually temporary.
- Cosmetic concerns: Mild asymmetry in biceps contour is possible, though tenodesis is specifically designed to minimize this.
How you can lower risk
- Protect the repair: Avoid resisted biceps curls and heavy gripping for at least 6 weeks. This is the single most important thing you can do.
- Follow the rehab protocol: Too fast risks failure; too slow risks stiffness. Stay on track with your physio.
- Stop nicotine: Supports tendon-to-bone healing.
- Report changes promptly: A sudden "pop," visible muscle shape change, or increasing pain should be reported immediately.
What are the risks of delaying or not pursuing surgery?
Your situation depends on symptom severity, the degree of tendon damage, your activity level, and whether other shoulder structures are involved.
Main risks of delaying (when symptoms are significant)
Ongoing pain and functional limitation
- Front-of-shoulder pain, night pain, and weakness with lifting/overhead activities can persist indefinitely if the tendon is significantly damaged.
- This disrupts sleep, work, exercise, and quality of life.
Progressive tendon damage
- A partially torn biceps tendon can progress to a complete tear (rupture). If the tendon retracts and the muscle shortens, tenodesis becomes more complex or may no longer be an option—leaving tenotomy (with its cosmetic and strength trade-offs) as the fallback.
Secondary shoulder problems
- An unstable or subluxating biceps tendon can irritate the rotator cuff and contribute to shoulder impingement, accelerating wear on other structures.
- Ongoing pain leads to altered movement patterns, which can cause neck, upper back, and opposite shoulder problems.
Medication dependence
- Relying on anti-inflammatories or repeated cortisone injections for months carries its own risks (tendon weakening from steroids, stomach and kidney issues from NSAIDs).
When watchful waiting can be reasonable
- Symptoms are mild and manageable with physio and activity modification.
- You're still improving with conservative treatment.
- The tendon damage is minor (mild tendonitis, no instability or significant tear).
When not to delay (seek assessment)
- Pain is significantly affecting your sleep, work, or sport despite trying conservative treatment.
- You notice weakness with lifting or overhead activities.
- You feel the tendon popping or clicking out of its groove.
- Your MRI shows a significant partial tear, subluxation, or SLAP tear that matches your symptoms.
- Your surgeon recommends tenodesis alongside another procedure (e.g. rotator cuff repair) and delaying means two separate surgeries later.
I still have questions
If you still have questions, please feel free to contact us directly.
Please note: Surgency is not a clinic itself. Nor can we help with emergency situations, or provide personalized medical advice—that is between you and your surgeon. If you are experiencing acute or severe symptoms, please present to your local emergency department or urgent care centre.
.avif)




