.png)
The information on this website is intended for informational purposes only and is not a substitute for medical, legal, or financial advice. Always consult a health provider, legal counsel, or financial professional if you have questions or concerns. The use of the information on this website does not create a physician-patient relationship between Surgency and you.
Surgency is a free resource for Canadian patients and caregivers. Private pathways Canadian physician in the public system to help you find the right surgeon for your needs.

As a family doctor in the public system, I believe transparency is a form of care. I created Surgency to help my patients struggling on long waitlists who wanted to understand all their options for timely medical attention.
Surgency is a free resource designed to empower and educate—helping you understand private pathways and find accredited surgeons within Canada. I hope Surgency brings you clarity.
Dr. Sean Haffey

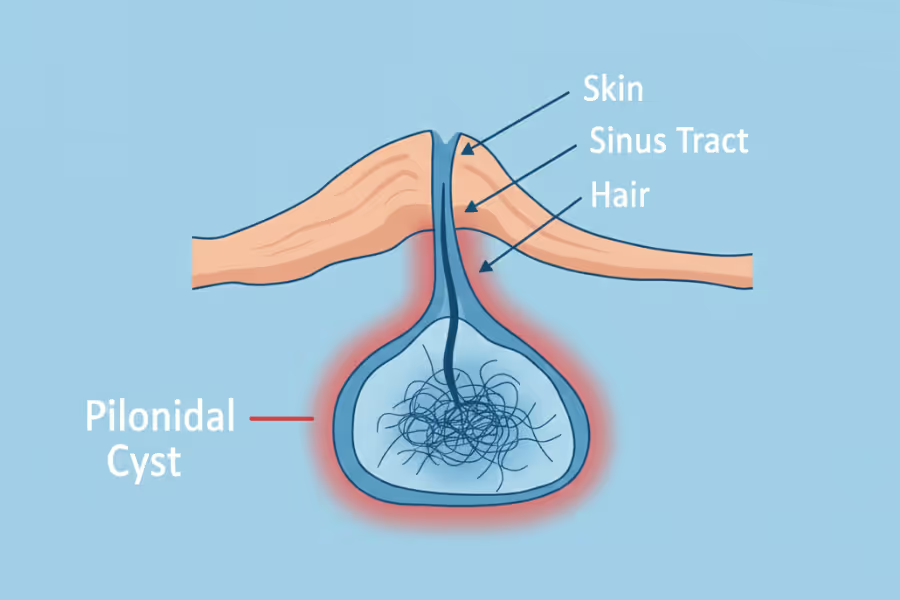
Sinus tract & fistulae excision is a surgical procedure that removes an abnormal tunnel (tract) that shouldn’t be there.
A sinus tract (not to be confused with your nasal sinus) is usually a channel that runs from a deeper pocket of chronic inflammation or infection to the skin surface, causing a persistent opening that can repeatedly drain fluid or pus.
A fistula is an abnormal connection between two body structures—for example, between the bowel/anal canal and the skin (common in perianal fistula), or between other tissues depending on the underlying cause.
In an excision, the surgeon aims to identify the tract, remove the chronically inflamed lining and any associated infected tissue, and then manage the wound so it can heal properly. Depending on the location and complexity, the surgeon may:
This surgery is different from simply treating flare-ups with antibiotics or draining an abscess. Those steps can reduce acute pain and pressure, but they may not remove the tract—so the problem can keep recurring.
Time matters when a tract or fistula is causing persistent drainage, recurrent infections/abscesses, odour, skin irritation, or ongoing pain. Private clinics can book assessment and treatment sooner—meaning less time managing dressings, antibiotics, and repeated flare-ups.
Going private can let you:
You know who will do the procedure, what the plan is, and what recovery will look like—often with clearer timelines for follow-up and wound care. A clear date also makes it easier to plan around school, work, and travel; and arrange time off.
Sinus tract and fistula surgery is often an outpatient procedure, typically taking 30–90 minutes depending on the complexity and location (e.g., pilonidal, perianal, or abdominal). Expect to be at the clinic or surgical centre for several hours including intake and recovery.

Your exact recovery plan comes from your surgeon, but here’s the general idea. Recovery is often slower than a simple cyst removal because the wound is frequently left open to heal.
What it feels like
Main goals
Typical instructions
What it feels like
Main goals
Typical steps
What it feels like
Main goals
Typical steps
Call your care team if you notice:
Sinus tract and fistulae surgery is generally more expensive than simple cyst removal because it is technically more difficult, often requires an operating room setting (rather than a simple procedure room), and may involve general anesthesia.
At private clinics, you can typically expect: $1,800 - $4,500+
Why the range?
Typical range: CA$4,000 - CA$10,000+
Why does the price vary so much?
In Canada, medically necessary sinus tract & fistulae excision care can be covered in the public system; private excision is typically out-of-pocket, though some extended plans may reimburse parts—ask for an itemized invoice.
Choosing your surgeon is one of the benefits of going private. Here’s how to choose wisely for sinus tract and fistulae surgery.
About the surgeon and plan
Technique and Strategy
Infection-specific questions
Recovery and costs
Sinus tract excision is usually not the first step if the issue is a one-time infection. It is something you consider when the tract is chronic, recurrent, or refusing to heal. Unlike cysts, fistulas rarely heal permanently on their own without intervention. Consult your doctor or surgeon to better understand your personal situation.
If the area keeps flaring or coming back
If you have chronic drainage
If it is interfering with daily life
If there is diagnostic clarity
Yes and no—you can reach out to any of the private surgeons listed on Surgency without a referral. Their intake teams are happy to answer questions, explain what they treat, share pricing ranges, and walk you through next steps.
However, to book a formal consultation with the surgeon, you'll typically need a referral from your family doctor or nurse practitioner. Don't have one? Many of the clinics can help coordinate a virtual GP appointment to get the referral paperwork sorted. All surgeons listed on Surgency offer virtual initial consultations, so you don't need to travel until you and the surgeon have agreed on a plan.
Before your consultation, expect the clinic to request relevant medical records and recent diagnostic imaging (X-ray, MRI, CT, ultrasound, lab work, etc.). Having these ready speeds up the process and lets the surgeon give you specific guidance on your very first call.
Your surgeon will give you a specific plan, especially regarding bowel preparation if the fistula is perianal.
Surgency is free for patients, funded for by surgeons.
Surgeons—who meet our listing criteria—pay a flat fee to list on the Surgency platform. To maintain objectivity, there are no commissions, referral fees, nor any ranking or recommending one surgeon over another.
Surgency is patient-first. Our goal is to make the process of finding a private surgeon as simple as possible. You choose who to contact. Learn more in our Advertising Policy.
Your situation depends on the tract’s location and cause (pilonidal vs. perianal vs. post‑surgical, Crohn’s-related, hidradenitis, etc.), how often it flares, and what imaging/exam shows. Some cases can be managed for a while, but chronic sinus tracts and fistulae often don’t fully resolve on their own—and delay can mean more cycles of infection and more complex disease. Always review your personal risks with your surgeon.
More flare-ups: swelling, pain, and drainage
Sinus tracts and fistulae often cycle between “quiet” and “active.” With delay, you may have more episodes of pain, swelling, and drainage—often with increasing disruption to work, exercise, travel, and sleep.
Higher chance of abscess and infection (and urgent visits)
A blocked fistula or tract can collect fluid and turn into an abscess, which may require urgent incision and drainage, antibiotics, or even emergency assessment. Repeated infections can also lead to repeated courses of antibiotics (and their side effects).
The tract can become more complex over time
Ongoing inflammation can lead to:
More scarring and harder surgery later
Repeated inflammation and prior drainages create scar tissue. That can:
Ongoing skin breakdown, odour, and constant wound care
Chronic drainage can irritate the surrounding skin, cause rashes and breakdown, stain clothing, and keep you in a constant routine of pads, gauze, and hygiene workarounds.
Impact on quality of life and mental load
Many people end up avoiding sitting, certain clothing, intimacy, swimming, or long days out because they can’t trust the drainage. The uncertainty (“Will it flare again this week?”) is a real burden.
Missing an underlying condition (the important one)
Not every draining opening is “just a tract.” Delaying workup can delay diagnosis or management of underlying causes such as:
Every surgery has risks. Your personal risk depends on your overall health, the tract’s location, depth, complexity, whether it’s inflamed/infected, and how closely you follow wound-care instructions. Review your specific situation with your surgeon.
If you still have questions, then feel free to contact us directly.
.avif)