.png)
The information on this website is intended for informational purposes only and is not a substitute for medical, legal, or financial advice. Always consult a health provider, legal counsel, or financial professional if you have questions or concerns. The use of the information on this website does not create a physician-patient relationship between Surgency and you.
Surgency is a free resource for Canadian patients and caregivers. Private pathways Canadian physician in the public system to help you find the right surgeon for your needs.

As a family doctor in the public system, I believe transparency is a form of care. I created Surgency to help my patients struggling on long waitlists who wanted to understand all their options for timely medical attention.
Surgency is a free resource designed to empower and educate—helping you understand private pathways and find accredited surgeons within Canada. I hope Surgency brings you clarity.
Dr. Sean Haffey

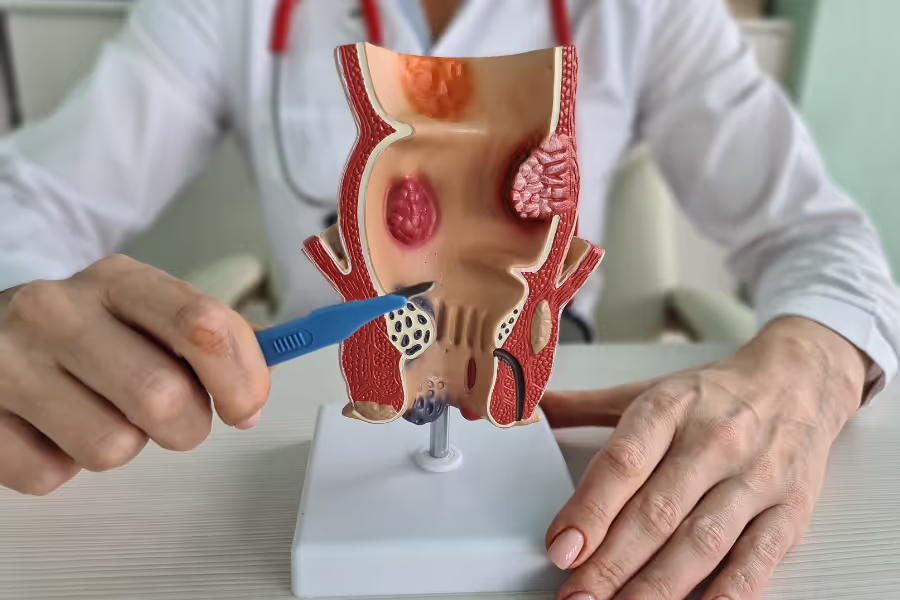
Hemorrhoid surgery is a procedure to treat swollen veins in the lower rectum or around the anus that cause bleeding, pain, itching, or lumps. When creams, fibre, or rubber band treatments aren’t enough, a surgeon can remove or shrink these veins so they stop bothering you.
There are a few ways to do it:
Most hemorrhoid surgeries take about 20–60 minutes. Plan a few extra hours at the centre for check‑in, anesthesia, and recovery before going home.
Basic steps

Every person heals differently—follow your surgeon’s plan. Taking the instructions seriously usually means a smoother recovery.
Week 1
Weeks 2–4
Weeks 5–8
Weeks 9–12+
In Canada, private clinics charge between $1,500 to $6,000 for hemorrhoid surgery. Higher end for multiple/external hemorrhoids, stapled procedures, or Doppler-guided/THD in premium facilities
Costs vary so much because of location, surgeon experience, facility type, complexity, and included services (some clinics offer all-inclusive, while others charge separately for anesthesia, followup care, etc.).
Choosing your surgeon is a major benefit of going private—use it to your advantage.
Hemorrhoid surgery isn’t for everyone, but it might be right for you if hemorrhoids keep bleeding, hurting, or prolapsing (bulging out) even after you’ve tried all the simpler stuff.
You’ve also tried conservative treatments without enough relief, like:
If those haven’t solved it—and symptoms are messing with school, sports, work, or sleep—surgery can remove or reduce the problem tissue so bleeding and prolapse stop. Talk to a colorectal or experienced general surgeon about your symptoms, what you’ve already tried, and which procedure (excisional, stapled, or Doppler‑guided/THD) fits your situation.
Yes and no—you can reach out to any of the private surgeons listed on Surgency without a referral. Their intake teams are happy to answer questions, explain what they treat, share pricing ranges, and walk you through next steps.
However, to book a formal consultation with the surgeon, you'll typically need a referral from your family doctor or nurse practitioner. Don't have one? Many of the clinics can help coordinate a virtual GP appointment to get the referral paperwork sorted. All surgeons listed on Surgency offer virtual initial consultations, so you don't need to travel until you and the surgeon have agreed on a plan.
Before your consultation, expect the clinic to request relevant medical records and recent diagnostic imaging (X-ray, MRI, CT, ultrasound, lab work, etc.). Having these ready speeds up the process and lets the surgeon give you specific guidance on your very first call.
Your surgeon will give specific instructions—follow their plan first.
Surgency is free for patients, funded for by surgeons.
Surgeons—who meet our listing criteria—pay a flat fee to list on the Surgency platform. To maintain objectivity, there are no commissions, referral fees, nor any ranking or recommending one surgeon over another.
Surgency is patient-first. Our goal is to make the process of finding a private surgeon as simple as possible. You choose who to contact. Learn more in our Advertising Policy.
Your individual risk depends on your health, the type/grade of hemorrhoids, the procedure used (excisional, stapled, Doppler‑guided/THD), anesthesia, and how closely you follow after‑care. Discuss your personal risks with your surgeon.
Your situation depends on your symptoms (bleeding, pain, prolapse), exam findings (grade of hemorrhoids, internal vs external), your daily demands (school, work, sport), and how well non‑surgical care works (fiber, stool softeners, creams, banding). Talk specifics with your surgeon.
Progressive symptoms and life impact
Disease progression
Harder treatment later
Emergency evaluations
Quality of life and mental health
Medication-related downsides
If you still have questions, then feel free to contact us directly.
.avif)


An experienced urogynecologist, and former President of the Alberta Society of Obstetricians and Gynecologists. Providing surgical and non-surgical treatments for prolapse, incontinence & cosmetic concerns.