

.png)


What is urethroplasty surgery?
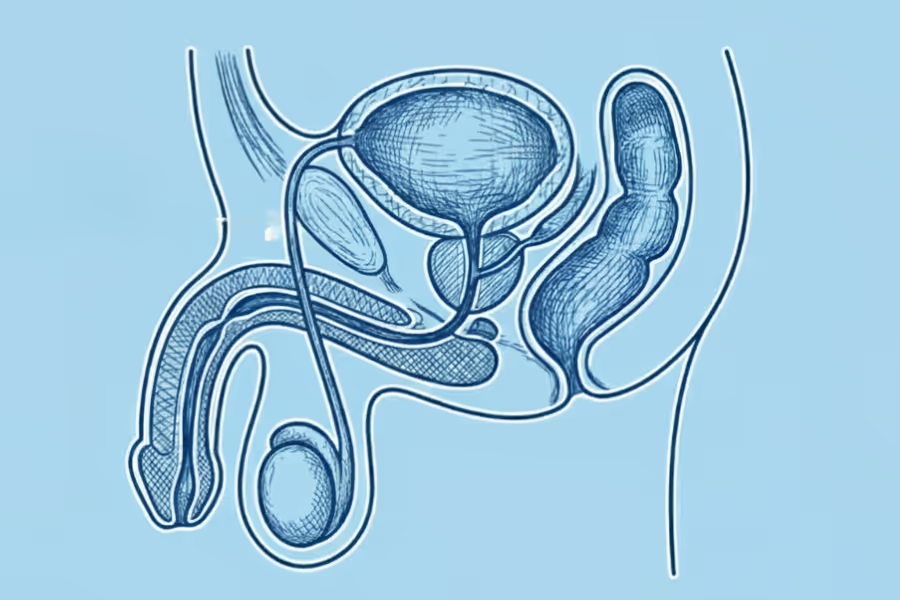
Urethroplasty is a surgery to fix a narrowed or blocked urethra—the tube that carries urine from your bladder out of your body. When this tube scars down (called a urethral stricture), the passage gets tight, and urine has to squeeze through a tiny space. That can lead to a weak stream, straining, taking forever to urinate, infections, or even urine backing up into the bladder.
In urethroplasty, the surgeon removes or opens up the scarred section and rebuilds the tube so urine can flow more normally again. Depending on how long and where the stricture is, your surgeon might:
- Choose for a less invasive procedure (e.g. direct vision internal urethrotomy)
- Simply cut out the damaged piece and reconnect the healthy ends, or
- Patch or rebuild the tube using a graft, often from the inside of your cheek (buccal mucosa).
The main goal is to give you a wider, stable urethra so urinating feels easier, more complete, and less stressful.
Urethroplasty procedures
Procedure TypeWhat It InvolvesWhen It Is UsedExcision and Primary Anastomosis (EPA)The surgeon cuts out the entire scar tissue segment and then sews the two healthy ends of the urethra back together.Used for short strictures (typically 3 cm or less) where the ends can be reconnected without tension. High success rate (~95%).Augmentation Urethroplasty (Graft/Flap)The stricture is cut open, and a patch of tissue (a graft, most often taken from the inside of the cheek, called Buccal Mucosa) is sewn onto the urethra to widen its diameter.Used for longer, more complex strictures where removing the segment would make re-connecting the ends too tight.Staged UrethroplastyA complex repair done in multiple surgeries over several months.Used for very long strictures, severe trauma, or strictures caused by skin diseases like Lichen Sclerosus (LS).
Why do Canadians get urethroplasty surgery done privately?
Shorter wait times
- Public wait lists for consults, cystoscopy, imaging, and OR time can be long.
- Private centres can often arrange assessment and surgery within weeks, not months.
- That means less time dealing with uncertainty, straining, and constant bathroom trips.
Choice and control
- Choose an experienced urethroplasty surgeon with specific experience in complex strictures.
- Pick the clinic location, schedule around exams, work blocks, or family plans.
- Talk through which technique fits you best (excision and re‑anastomosis vs graft urethroplasty) and your anaesthesia preferences.
Peace of mind
- You know who is operating, what they plan to do, and when it will happen.
- Clear timelines and an itemized quote make it easier to organize time off, travel, and support.
- Direct communication and quick sharing of results cut down “waiting in the dark.”
Preventing further problems
- Ongoing strictures can mean infections, bladder strain, and, in some cases, kidney issues or emergency retention.
- Earlier urethroplasty can restore better flow, reduce urgent trips to the bathroom, and lower the need for repeated dilations or ER visits.

Urethroplasty surgery: what to expect
Surgery usually about 2–4 hours, depending on how long the stricture is, where it is in the urethra, whether you need a graft. Expect to be in clinic most of the day for check‑in, anaesthesia, surgery, and early recovery.
Basic steps (what actually happens)
1. Check‑in and planning
- You meet the nurse, anaesthesia team, and surgeon.
- They review your history, imaging, and previous tests.
- The plan is confirmed: where the stricture is, what type of urethroplasty they expect to do, and what graft (if any) might be needed.
2. Anaesthesia
- You almost always get general anaesthesia, so you’re fully asleep.
- Sometimes a spinal/epidural is added for extra pain control.
3. Position and prep
- You’re positioned on a padded table so the surgeon can reach the urethra and, if needed, your mouth (for a cheek graft).
- The skin is cleaned with antiseptic and covered with sterile drapes.
4. Accessing the urethra
- A careful incision is made in the perineum (the area between the scrotum and anus) or along the penis, depending on where the stricture is.
- The surgeon gently exposes the urethra while protecting nearby nerves and blood vessels.
5. Finding and opening the stricture
- The urethra is opened to directly see the scarred, narrowed segment.
- The tight area is either:
- Cut out and the healthy ends are re‑joined (excision and primary anastomosis), or
- Opened up and then patched or rebuilt using a graft.
6. Graft (if needed)
- For longer or more complex strictures, the surgeon may:
- Take a thin graft from the inside of your cheek (buccal mucosa), or
- Use another suitable tissue.
- This graft is sewn onto the urethra to widen and rebuild the tube.
7. Rebuilding the urethra and placing a catheter
- The urethra is carefully closed and reshaped around a catheter so the new passage is the right size and shape.
- A urinary catheter (and sometimes a second suprapubic catheter through the lower abdomen) is left in place to let the repair heal.
8. Closing and dressing
- Deeper layers and skin are closed with stitches.
- Dressings are applied, and the catheter is secured.
9. Wake‑up and early recovery
- You wake up in a recovery area.
- The team checks your breathing, pain, and catheter position.
- You get early instructions about moving carefully, catheter care, and what to expect over the next few days.

What can I expect from the recovery process?
Urethroplasty is a bigger surgery than a simple scope or dilation, so expect recovery to be a bit of a process. Everyone heals differently, follow your surgeon’s plan.
First few days (Days 1–3)
What it feels like
- Sore and bruised between the legs (perineum), sometimes inside the mouth if you had a cheek graft
- You’ll have a catheter draining urine
Main goals
- Control pain and swelling
- Protect the incision and catheter
Typical activities
- Short, careful walks around the house
- Rest with hips relaxed; avoid big stretches or sudden movements
- Keep the incision clean and dry as instructed
Days 4–14
What it feels like
- Soreness is still there but slowly settling
- Sitting on hard chairs can feel uncomfortable or “pressure‑y”
Main goals
- Move comfortably without pulling on the repair
- Take care of the catheter and mouth (if graft used)
Typical activities
- Light daily tasks and desk/school work from home if you feel up to it
- Gentle walking, but no running, heavy lifting, or sports
- Quick showers usually OK once your surgeon says so (no baths or hot tubs)
- Regular catheter care and drinking enough fluids
Weeks 3–6
What it feels like
- Discomfort continues to improve
- You’ll likely have a catheter check or imaging (like a urethrogram) to see how the repair is healing
Main goals
- Make sure the new urethra is healing well
- Gradually get back to more normal routines
Typical activities
- If your test shows things look good, the catheter may be removed
- Back to most normal walking and light activities
- Many people can return to non‑physical school or desk work if they haven’t already
Weeks 6–12 and beyond
What it feels like
- Urinating should feel easier and more “normal” than before surgery
- Energy levels and comfort keep improving
Main goals
- Build back full confidence with urinating and movement
- Slowly return to sport, heavier work, or the gym (when cleared)
Typical activities
- Gradual return to:
- Running or more intense cardio
- Gym and job duties that involve lifting or being on your feet
- Follow‑up visits to check that the urethra is staying open and you’re happy with the result
Red flags – call your team right away
Anytime after surgery, contact your surgeon or go for urgent care if you have:
- Fever, chills, or feeling very unwell
- Worsening redness, swelling, or pus‑like drainage from the incision
- Catheter not draining, sudden trouble urinating, or severe bladder pain
- Big increase in pain, especially in the perineum or groin
- New calf pain/swelling or chest pain/shortness of breath
Recovery from urethroplasty is about being patient: protect the repair, respect the catheter, and follow your surgeon’s timeline, even if you feel better sooner.
How much does urethroplasty surgery cost in Canada?
For private care in Canada, urethroplasty is a major reconstruction, so it’s on the higher side. And the cost varies substantially based on the procedure type (excision and primary anastomosis, graft/flap, staged), location, surgeon expertise, anesthesia.
In Canada, private centres charge roughly $15,000–CA$30,000+
- The exact number depends on:
- How complex/long the stricture is
- Whether you need a cheek graft
- OR time and facility type (clinic vs hospital partnership)
How much does it cost in the United States on average?
In the U.S., you can expect between CA$15,500 - $30,000+
What’s usually included
Most bundled quotes typically cover:
- Surgeon fee (and assistant, if used)
- Anaesthesia and monitoring (usually general anaesthesia)
- Accredited facility/OR fees, nursing, and standard supplies
- Use of surgical equipment (e.g., loupes/magnification, instruments, catheter placement)
- Immediate post‑op recovery care
- At least one routine follow‑up visit to check healing and review early results
What’s often not included
These may be billed separately or handled outside the package:
- Initial consults and pre‑op tests (cystoscopy, uroflow, imaging, lab work)
- Extra OR time beyond the booked block or an unplanned overnight stay
- Prescriptions after surgery (pain meds, antibiotics, stool softeners)
- Later imaging or flow tests beyond the standard follow‑up protocol
- Travel and accommodation if you’re coming from another province or country
Tips to compare quotes
- Ask for line items: surgeon fee, facility, anaesthesia, and any special equipment.
- Confirm:
- What happens if the surgery is more complex than expected
- How many follow‑ups are included
- Whether catheter removal and post‑op tests are part of the package.
Choosing a surgeon and clinic
Choosing your surgeon is one of the benefits of going the private route. Here's how to choose wisely.
What to look for
Experience and volume
- Ask how many urethroplasties they do per year.
- Ask if they routinely handle:
- Longer strictures
- Redo surgeries
- Graft (buccal mucosa) cases
- Higher volume usually means more refined technique and smoother pathways.
Credentials and training
- Confirm they’re licensed with your provincial college (CPSO, CPSBC, CPSA, CMQ, etc.).
- Look for an FRCSC‑certified urologist with specific training or focus in:
- Reconstructive urology
- Urethral surgery / trauma
Technique and tools
- Ask which techniques they use (EPA, graft/patch, staged repairs) and which they recommend for you.
- Ask how they decide when to use a cheek graft and how they harvest it.
- Check that they use proper imaging and scopes before surgery to plan the repair.
Outcomes and safety
- Ask for recent stats, like:
- Stricture recurrence rates
- Infection or complication rates
- How often patients need another procedure
- A good surgeon should be comfortable talking about numbers and trade‑offs.
Pre‑op and after‑care
- You want a clear plan for:
- Pre‑op tests (cystoscopy, uroflow, imaging, bloodwork)
- How long the catheter will stay in
- When you’ll have imaging/flow tests after surgery
- How to reach the team if you’re worried
Facility quality
- Prefer an accredited hospital or surgical centre (Accreditation Canada, CAAASF, or provincial equivalent).
- Ask about:
- Consistent anaesthesia coverage
- Access to imaging and emergency backup if something unexpected happens
Pricing transparency (for private care)
- Ask for an itemized quote:
- Surgeon fee
- Facility fee
- Anaesthesia
- Graft/extra supplies
- Follow‑ups and any imaging/cystoscopy included
Questions to ask in your urethroplasty consult
About the surgeon and plan
- How many urethroplasties do you perform each year, and what types (EPA, graft, staged)?
- What does my imaging show exactly, and which technique do you recommend for me and why?
- What is your approximate recurrence rate over the last few years?
Anaesthesia and logistics
- What kind of anaesthesia will I have, and what’s the pain‑control plan afterwards?
- Will I stay overnight, or is it same‑day discharge?
Recovery and follow‑up
- How long will the catheter stay in, and how is it removed?
- When can I return to school/desk work, more physical jobs, and sport/gym?
- What red flags should make me call you or go to the ER?
Costs and documentation (if private)
- What exactly is included in my quote, and what could add extra cost?
- If you have to change the plan mid‑surgery, how is that handled for consent and pricing?
- Will I get a written report and after‑care plan to share with my family doctor?
A strong urethroplasty program is open about results, clear about the plan, easy to reach with questions, and totally transparent about what you’re paying for.
If you're currently interested in private surgical pathways within Canada, you can click here for a list of providers.

Urethroplasty surgery frequently asked questions
How do I know if varicocele surgery is right for me?
Figuring out if urethroplasty is right for you starts with what’s actually going on in your urethra, not just how annoying your stream feels. Your urologist will connect your symptoms, tests, and goals.
Urethroplasty might be right if,
- You have clear symptoms of a stricture, like:
- Weak or split stream
- Straining to urinate, taking forever
- Starting and stopping mid‑urination
- Feeling like you never fully empty
- Tests prove there’s a narrowing, for example:
- Cystoscopy (camera in the urethra)
- Imaging (retrograde urethrogram, voiding study)
- You’ve already tried simpler options and they’re not working, like:
- Repeated dilations or internal urethrotomy
- Catheter changes / temporary fixes
Common reasons people get urethroplasty:
- Constant urinary symptoms that mess with school, work, sleep, or travel
- Recurrent urinary infections from poor emptying
- Needing catheters or emergency care for urinary retention
- Wanting a more durable, long‑term fix instead of endless dilations
When urethroplasty might not be right (yet)
- Mild symptoms with a small, stable stricture that isn’t really affecting your life
- A first‑time, short stricture that responds well to a simple procedure (your urologist may still suggest trying that first)
- Active infection, uncontrolled health issues, or you’re not cleared for anaesthesia right now
Do I need a referral?
Yes and no—you can reach out to any of the private surgeons listed on Surgency without a referral. Their intake teams are happy to answer questions, explain what they treat, share pricing ranges, and walk you through next steps.
However, to book a formal consultation with the surgeon, you'll typically need a referral from your family doctor or nurse practitioner. Don't have one? Many of the clinics can help coordinate a virtual GP appointment to get the referral paperwork sorted. All surgeons listed on Surgency offer virtual initial consultations, so you don't need to travel until you and the surgeon have agreed on a plan.
Before your consultation, expect the clinic to request relevant medical records and recent diagnostic imaging (X-ray, MRI, CT, ultrasound, lab work, etc.). Having these ready speeds up the process and lets the surgeon give you specific guidance on your very first call.
How do I prepare?
Your urologist’s instructions come first—follow their plan if it differs.
1. Get your health and meds organised
- Stop nicotine if you can. Smoking or vaping slows healing and raises infection risk, so quitting 4+ weeks before surgery really helps.
- Itemize everything you take—prescriptions, Advil/aspirin, vitamins, herbal supplements—and give that list to your team. They may ask you to pause blood thinners, some anti‑inflammatories, or certain herbals that increase bleeding (only if your doctor says so).
- Try to go into surgery in decent shape: regular sleep, good hydration, and simple balanced meals with some protein.
- Expect pre‑op tests like bloodwork, urine tests, and imaging (often a urethrogram) and possibly medical clearance if you have other conditions.
2. Set up your home “recovery zone”
- Have loose joggers/shorts that fit over bandages and a catheter, plus comfortable underwear that can hold dressings in place.
- In the bathroom, keep gentle soap, clean towels, and a small bin for used dressings or catheter supplies.
- Pick a spot to rest where you can easily reach water, your phone and charger, your meds, and something to watch or listen to.
3. Plan support and logistics
- Arrange a ride home (you cannot drive after anaesthesia) and, if possible, someone to stay with you for the first 24 hours.
- Plan time off school/work, especially if your job is physical; tell teachers or your employer you’ll need lighter duties at first.
- If you’re travelling for surgery, confirm which follow‑ups can be virtual, and sort out where you’ll stay and how you’ll get to the clinic.
4. Know your surgery‑day plan
- Follow fasting rules exactly: no food after the time they give you, and only clear fluids up to the cut‑off if allowed.
- Shower the night before and the morning of surgery, avoid lotions or powders near the area, and do not shave—the team will handle any hair if needed.
- Bring your health card/ID, medication list, glasses/contact case if needed, and loose, easy‑on clothes for going home.
5. Prepare for pain and bathroom issues
- Fill your pain prescriptions before surgery if you can, and have acetaminophen (and any other surgeon approved meds) ready at home. Take them on schedule at first instead of waiting until the pain is intense.
- Because pain meds can cause constipation, have a fibre supplement or stool softener ready and drink plenty of water, so you are not straining on the toilet.
How much does Surgency cost?
Surgency is free for patients, funded for by surgeons.
Surgeons—who meet our listing criteria—pay a flat fee to list on the Surgency platform. To maintain objectivity, there are no commissions, referral fees, nor any ranking or recommending one surgeon over another.
Surgency is patient-first. Our goal is to make the process of finding a private surgeon as simple as possible. You choose who to contact. Learn more in our Advertising Policy.
What are the risks involved?
Your personal risk depends on your health, where the stricture is, how long it is, which urethroplasty technique is used, and how closely you follow after‑care. Your urologist will be in a better position to understand your personal situation.
Common and usually temporary
These are uncomfortable but expected for many people:
- Pain, swelling, and bruising in the perineum (area between scrotum and anus) and sometimes at the cheek if a graft is taken
- Soreness or pressure when sitting for the first days to weeks
- Nausea, grogginess, or headache from anaesthesia; constipation from pain meds
- Numbness or tingling near the incision, or around the scrotum/inner thigh
- Small firm “healing lumps” under the skin that soften over time
Less common risks
These happen less often, but you should know about them:
- Wound infection or skin irritation around the incision
- Haematoma (a pocket of blood) or fluid build‑up that makes the area look puffy or tight
- Irritated nerves near the urethra or perineum, causing sensitive spots or “electric shock” feelings that take time to calm down
- Mouth discomfort where the cheek graft was taken: tightness, soreness, or temporary numb areas
- Scar tissue forming again in the urethra, causing partial recurrence of the stricture
Procedure‑specific issues
Because urethroplasty is a reconstruction, there are some special considerations:
- The repair can narrow again over time and sometimes needs another procedure (dilation, internal cut, or repeat urethroplasty)
- In graft cases, the cheek site can rarely have longer‑lasting numbness or tightness
- Some people notice a change in the direction or shape of the urine stream even when flow is much better overall
Uncommon but important risks
These are rare, but serious:
- Significant bleeding that needs a return to the OR or extra procedures
- Deep infection around the repair
- Blood clots in the legs or lungs (DVT/PE), which can happen after any bigger surgery if you are not moving much
- Major damage to surrounding structures (like the erectile tissue) is uncommon in experienced hands, but can affect erections or cause leakage if it occurs
How you can lower your risk
You can’t remove all risk, but you can tilt things in your favour:
- Stop nicotine before surgery, and follow all pre‑op medication and fasting instructions
- Keep the incision clean and dry; follow catheter‑care directions exactly
- Avoid heavy lifting, straining, or “testing” the repair too early
- Walk short distances as allowed to keep blood moving and reduce clot risk
- Take pain and antibiotic meds exactly as prescribed
Red flags
Fever or chills, spreading redness or pus from the wound, catheter not draining, sudden trouble urinating, rapidly increasing swelling, severe pain that’s not controlled by meds, calf pain or shortness of breath. If these show up, contact your team or go to urgent care/ER.
Urethroplasty is a major but well‑established surgery. In experienced hands, most problems are mild and temporary, and the main goal is a more reliable, long‑term fix for your stricture.
What are the risks of delaying or not pursuing surgery?
Your situation depends on how bad your urinary symptoms are, what tests show (location/length of the stricture), your goals (comfort, avoiding catheters, long‑term fix), and how well simpler treatments work (dilations, temporary scopes, meds). Talk details with your urologist.
Main risks of delaying or not having urethroplasty
(when symptoms or tests are significant)
Progressive symptoms and limits
If the narrowing stays or worsens, you may have:
- Increasingly weak or split stream, straining, and taking ages to urinate
- More trips to the bathroom, including at night
- Rising stress about going anywhere without easy toilet access
Some people end up needing repeated emergency visits for urinary retention (not being able to urinate at all).
Bladder and kidney strain
When urine can’t flow out properly, it can back up:
- The bladder walls thicken and become less stretchy over time
- Pressure can travel up toward the kidneys, risking damage in more severe, long‑term cases
- Incomplete emptying raises the chance of recurrent urinary infections
Harder problem to treat later
A long‑standing, untreated stricture can:
- Become denser and longer, making surgery more complex
- Have a higher chance of needing grafts or staged repairs
- Be less likely to respond to quick fixes like dilation or internal cuts
The longer abnormal urination patterns go on, the harder they can be to fully “reset,” even after surgery.
Quality‑of‑life drag
Living around a stricture can mean:
- Planning your day around toilets and avoiding long trips or events
- Embarrassment about slow urination, especially in public washrooms
- Sleep disruption from night‑time trips and a constant low‑level worry about “getting stuck”
Over time, this can wear on mood, energy, and confidence.
Medication and short‑term fix downsides
Relying on repeated dilations or temporary procedures instead of a more durable repair can mean:
- Frequent clinic or hospital visits
- More scarring each time in some cases
- Ongoing use of antibiotics and pain meds, with their own side‑effects
When watchful waiting can be reasonable
Delaying urethroplasty may be okay if:
- Symptoms are mild, and you can urinate safely without major straining or retention
- The stricture is short and stable on tests
- You and your urologist have a clear plan for monitoring (symptom review, flow tests, imaging) and you’re comfortable with the trade‑offs
When it’s usually not wise to keep delaying
You and your urologist should talk seriously about surgery if:
- You’ve had repeated episodes of retention, or you rely on catheters
- You have frequent urinary infections or bladder/kidney changes on tests
- Urinating is a daily struggle that limits school, work, travel, or sleep
- Dilation or internal cuts keep failing or the stricture is clearly getting longer/tighter
Urethroplasty isn’t for every minor narrowing. But if a significant stricture is repeatedly causing blockage, infections, or emergencies, timely reconstruction can protect your bladder and kidneys and make everyday life much easier.
I still have questions
If you still have questions, then feel free to contact us directly.
.avif)

